
You eat well. You exercise. Your cholesterol report looks “fine.”
So why do some people who seem perfectly healthy still end up with a sudden heart attack or stroke?
Because for a portion of the population, heart risk isn’t just lifestyle-related — it’s inherited, and it can stay quiet for years. Standard cholesterol tests are helpful, but they don’t always reveal the full picture of what’s happening inside your arteries.
The Blind Spot in Routine Cholesterol Checks

Doctor highlighting heart and ECG symbol for cardiology screening.
Most routine lipid panels focus on familiar numbers: total cholesterol, LDL, HDL, and triglycerides.
These markers matter — but they mainly describe cholesterol levels in broad terms. What they may miss is the type and number of cholesterol-carrying particles, and whether you carry genetic lipid traits that accelerate plaque build-up even when your usual readings look acceptable.
In other words: two people can have the same LDL level, but very different cardiovascular risk — depending on what’s happening beneath those headline numbers.
The Genetic Marker Many People Don’t Know About: Lipoprotein(a)
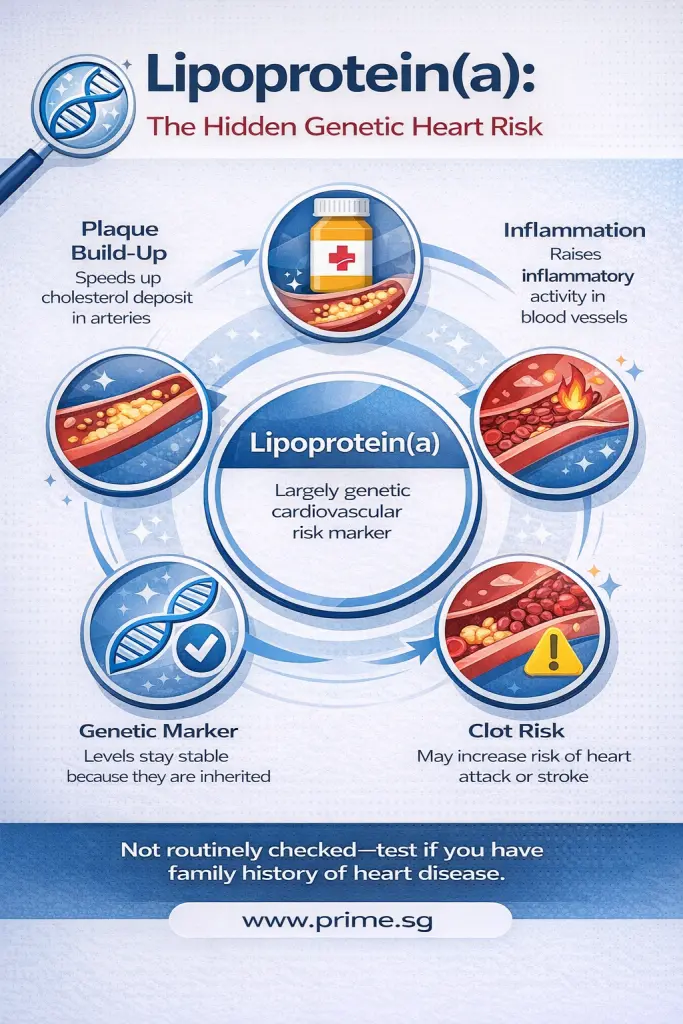
The Genetic Marker Many People Don’t Know About: Lipoprotein(a) Infographics
One of the most important “hidden” markers is Lipoprotein(a), commonly written as Lp(a).
Lp(a) is largely determined by genetics — meaning you can inherit a high level even if you’re slim, active, and disciplined with food. And unlike many lifestyle-related markers, Lp(a) may not improve meaningfully with diet or exercise alone.
Why it matters
High Lp(a) doesn’t just “sit there” on a lab report — it can actively contribute to cardiovascular disease in more than one way:
1) It can accelerate plaque build-up
Lp(a) is considered more atherogenic (more likely to promote plaque) because it can encourage cholesterol to deposit in the artery wall, contributing to narrowing over time.
2) It is linked to inflammation
Higher Lp(a) levels are associated with greater inflammatory activity within blood vessels. Inflammation plays a key role in making plaques more unstable — which matters because unstable plaques are more likely to rupture.
3) It may increase clot tendency
One reason Lp(a) draws so much attention is its association with clot-related processes. When a plaque ruptures, clot formation can quickly block blood flow — leading to heart attack or stroke.
4) It often stays “stable” for years
Unlike LDL, which can shift with lifestyle and medication, Lp(a) levels tend to remain relatively stable long-term because genetics drive it. That’s why testing can be useful: you often don’t need repeated checks unless your doctor advises.
The tricky part: many people don’t know they have elevated Lp(a) because it’s not routinely included in standard screening panels.
Why Lp(a) Does Not Always Show Up in Standard Cholesterol Results
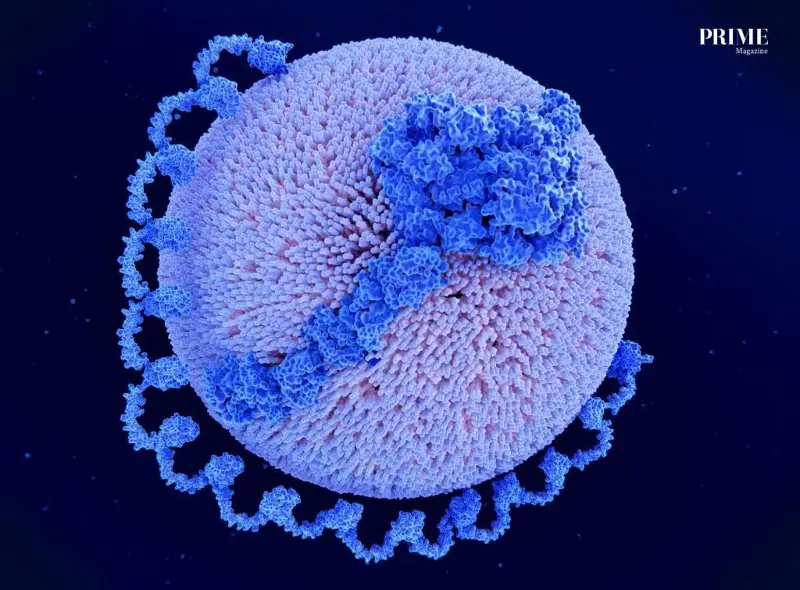
Lipoprotein A Particle Illustration
This is a common misunderstanding: people assume that if their LDL is normal, Lp(a) must also be normal — but Lp(a) is not automatically “captured” by routine cholesterol readings.
Here’s why:
- Lp(a) is a specific type of lipoprotein particle, not a separate line item in most standard lipid panels.
- Routine tests measure LDL as a broad category — and Lp(a) can be present even when LDL appears acceptable.
- In some lab calculations, Lp(a) cholesterol may be partly included inside the LDL number, but you still won’t know it’s there unless Lp(a) is measured directly.
- Most importantly, the risk associated with Lp(a) isn’t only about “how much cholesterol” it carries — it’s also about its genetic structure and its inflammatory/clot-related effects.
So a “good” cholesterol report can still miss a meaningful inherited risk driver.
How Is Lp(a) Tested?
Lp(a) is checked through a specific blood test.
What to know:
- It’s a simple blood draw, like other cholesterol-related tests.
- Fasting is not always required (requirements vary by clinic/lab, so follow your doctor’s instructions).
- Because Lp(a) is relatively stable and genetically driven, many people only need a once-in-a-lifetime test, especially if the reason for testing is family history.
- Your doctor will interpret the result based on the lab’s reporting unit and your overall risk profile (family history, blood pressure, diabetes, smoking, age, and more).
If you’ve never had it tested, you won’t know where you stand — and that’s the main issue.
Who Should Consider Testing?

Blood sample tube for lipid profile and cholesterol testing.
If you have a family history of early heart disease, it may be worth discussing Lp(a) testing even if you feel well.
In particular, consider it if:
- a close family member had heart disease at a younger age
- men in the family developed heart disease before 55
- women in the family developed heart disease before 65
This is one of those cases where “I feel fine” doesn’t always equal “I’m low risk.”
Lp(a) Isn’t the Only “Advanced” Clue
Lp(a) is part of a bigger category of markers that help doctors assess risk beyond LDL alone. Another key indicator is ApoB.
ApoB: The particle count that LDL doesn’t tell you
ApoB (Apolipoprotein B) is found on the surface of the particles most likely to contribute to plaque — including LDL and other atherogenic lipoproteins. That makes ApoB a useful way to estimate how many plaque-forming particles are circulating in your blood.
Why that matters:
- You can have “normal LDL” but still have a high number of atherogenic particles, especially if your LDL particles are smaller/denser.
- More particles mean more opportunities for cholesterol to enter the artery wall.
- ApoB can help explain why some people with acceptable LDL still show early plaque on scans — while others do not.
Small, dense LDL: Why “type” can matter
Some people have LDL particles that are smaller and denser, which may be more likely to penetrate artery walls and contribute to plaque formation. This is one reason advanced testing can add clarity when the standard panel doesn’t match someone’s personal or family history.
These aren’t buzzwords — they’re tools that can explain why two people with similar LDL can have very different risk profiles.
If Your Results Are High, What Happens Next?
The goal isn’t to panic — it’s to reduce total cardiovascular risk.
Depending on your overall risk factors, your doctor may focus on:
- tighter control of blood pressure and blood sugar
- more structured cholesterol-lowering strategies when appropriate
- lifestyle changes that reduce inflammation and improve metabolic health
- closer monitoring for early cardiovascular warning signs
Sometimes, even if LDL doesn’t look “high” by standard cut-offs, a more proactive approach may be recommended — because the real target is risk reduction, not chasing a single number.

Women’s Aerobics Class
Lifestyle Still Counts — Even When Genetics Don’t Budge
Lipoprotein Text Printed on Paper
Even if Lp(a) is genetic, lifestyle still plays a powerful supporting role:
- consistent aerobic exercise + resistance training
- balanced eating patterns lower in saturated fats and added sugars
- better sleep quality
- stress management
These steps can improve triglycerides, HDL, insulin sensitivity, and inflammation — all of which affect long-term heart outcomes. Lifestyle may not “erase” genetic risk, but it can reduce the chances that multiple risks stack up at the same time.
A Smarter Way to Screen
If heart disease runs in your family, don’t let a “normal cholesterol” label give you false reassurance. Ask whether advanced lipid markers — especially Lp(a) and ApoB — should be part of your screening. PRIME